
Description
Losing weight has less to do with the amount of calories you eat or how much you exercise, and everything to do with hormone balance, cortisol levels, and metabolism.
By looking at the hidden inflammatory triggers and hormone imbalances we can discover what is holding you back from the body you want and the results you deserve.
All at-home lab tests take 3-4 weeks to get the results back after you’ve mailed them in. At that time you will receive a wellness plan, which includes:
- Customized Nutritional Supplement Plan
- Dietary Guidance
- Detoxification Methods
- Lifestyle Changes
- Sleeping Tips
- Stress Reduction Techniques
- Goal Setting Formula Sheet
- Progress Report Tracking
- Private FB Support Group Access
Weight Loss Coaching Call
Plus, included in this package you’ll receive a coaching call with one of Dr. Cabral’s Certified Health Coaches to review your results and wellness recommendations.
Take back control of your health & body!
FAQ
- We will mail you lab test kit out to you within 48 hours of your purchase (M-F).
- Coaching calls are scheduled for approximately 3-4 weeks after you complete and mail in your lab kit.
- Your personalized health recommendations do not include the cost of recommended food lists or products.
- Health coaching calls are completed by Dr. Cabral’s personally certified Holistic Health Coaching Team.
- During your health coaching call you will receive an explanation of your labs, as well as a specific plan for you.
- After your consultation is over you will be sent a private link from your health coach for additional bonus reports
- Any statements or claims about the possible health benefits conferred by any foods or supplements have not been evaluated by the Food & Drug Administration and are not intended to diagnose, treat, cure or prevent any disease.
What is Included in the Profile?
Estradiol (E2)
At optimal physiological levels in women promotes a healthy distribution of fat in hips, thighs, breasts, and subcutaneously. However, in excess, and in the absence of progesterone, estrogen predisposes to unhealthy surplus weight gain in these tissues. Men generally have much lower levels of estradiol and higher testosterone, which is responsible for greater muscle mass and less fat distribution in areas of the body normally seen in women. In overweight men testosterone levels drop and estrogens rise leading to the same problematic weight gain in the hips, thighs, and breasts (referred to as gynecomastia) as seen in women.
Progesterone (Pg)
In addition to its primary role in attenuating the effects of excess estrogen in the body by downregulating estrogen receptors, aids weight management by acting as a natural diuretic. Its natural calming effects in the brain may also reduce stress-related overeating and food cravings. As a mineralocorticoid receptor antagonist, progesterone counteracts the effects of mineralocorticoid activation, which include the stimulation of fat cell formation, increased body weight, and release of inflammatory cytokines. However, excessive supplementation with progesterone to higher than normal levels can increase appetite and also slow the rate of food emptying from the stomach and moving through the digestive tract, causing slower digestion and bloating.
Testosterone (T) and DHEA-S (DS)
These are androgens that increase lean muscle mass and metabolic rate. As androgen levels decline, muscle mass also decreases with a corresponding increase in adiposity. Low androgens can also reduce vitality and tolerance for exercise. Weight gain itself, with its resulting hormone imbalances, can trigger a drop in testosterone as the aromatase enzyme within fat tissue converts androgens to estrogens. In men this contributes to a female-type body fat distribution, including breast tissue development. In women with polycystic ovarian syndrome (PCOS), high testosterone and DHEA are linked to insulin resistance and weight gain, particularly in the abdomen.
Cortisol (C)
Imbalances can create problems with blood sugar control, sleep patterns, appetite, food cravings, and tolerance exercise. Under stress, excessive cortisol production particularly in concert with insulin, promotes fat storage in abdominal adipose tissue. This visceral type of fat is closely associated with insulin resistance and metabolic syndrome and thus more hazardous to health. Chronically elevated cortisol is a known risk factor for pre-diabetes and cardiovascular disease.
Thyroid Stimulating Hormone (TSH)
Elevations, even within the high-normal range, are linked with hypothyroidism, low metabolic rate and obesity. Hypothyroidism is linked to elevated cortisol and can also be a consequence of oral estrogen therapy, which increases the production of binding proteins that reduce thyroid hormone bioavailability
Vitamin D (D2, D3)
Deficiency is common in obesity and particularly associated with hyperinsulinemia and visceral fat. Whether by cause or effect, identifying and correcting vitamin D3 deficiency may improve insulin sensitivity
Fasting Insulin (In)
Fasting nsulin when elevated, is a marker of insulin resistance which precedes metabolic syndrome, PCOS, and type 2 diabetes. Increased levels, particularly in concert with cortisol lead to central obesity and increased inflammatory and other cardiovascular disease markers. Hyperinsulinemia also contributes to decreased testosterone levels in men, but increased testosterone and decreased ovulation in women.
Hemoglobin A1c (HbA1c)
This marker is an indirect measure of the average circulating glucose levels over the previous three months. An HbA1c of more than 6% is predictive of type 2 diabetes and cardiovascular disease risk.
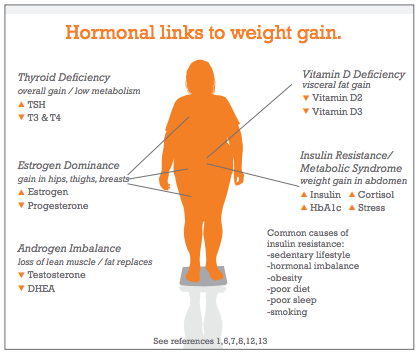
Hormone Weight Gain Connection
Estrogen/progesterone imbalance: weight gain in hips, thighs; water retention; low thyroid/metabolism
Testosterone/DHEA imbalance: decreased lean muscle, low metabolic rate; abdominal obesity
Cortisol imbalance: increased appetite, sugar cravings, and belly fat; inhibits thyroid and metabolism
Vitamin D3 deficiency: hyperinsulinemia; visceral fat
TSH elevated: hypothyroidism, low metabolic rate, obesity
Fasting Insulin: insulin resistance, abdominal obesity
HbA1c: predictive of type 2 diabetes
To date this is the most comprehensive Functional Medicine lab test to find out the underlying root causes of why you gain weight and can’t keep the weight off!
SAMPLE REPORT:
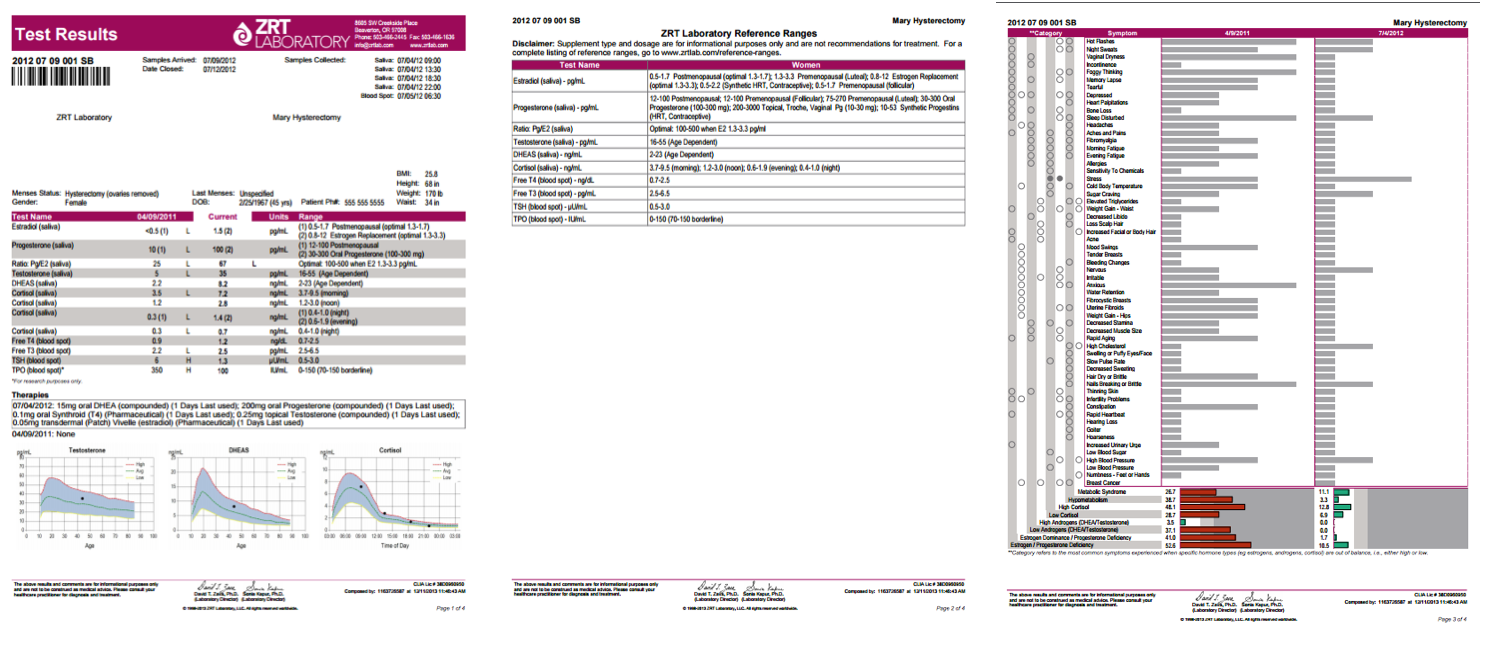
For More Details Watch the Video Below
References
1. Björntorp P. The regulation of adipose tissue distribution in humans. Int J Obes Relat Metab Disord. 1996;20(4):291-302.
2. McTiernan A, Wu L, Chen C, et al. Women’s Health Initiative Investigators. Relation of BMI and physical activity to sex hormones in postmenopausal women. Obesity (Silver Spring). 2006;14(9):1662-77.
3. Pasquali R, Vicennati V, Gambineri A, Pagotto U. Sex-dependent role of glucocorticoids and androgens in the pathophysiology of human obesity. Int J Obes (Lond). 2008;32(12):1764-79.
4. Shi H, Seeley RJ, Clegg DJ. Sexual differences in the control of energy homeostasis. Front Neuroendocrinol. 2009;30(3):396-404.
5. Torréns JI, Sutton-Tyrrell K, Zhao X, et al. Relative androgen excess during the menopausal transition predicts incident metabolic syndrome in midlife women: study of Women’s Health Across the Nation. Menopause. 2009;16(2):257-64.
6. http://www.endotext.org/section/obesity/; Part 12: Endocrine changes in obesity.
7. Knudsen N, Laurberg P, Rasmussen LB, et al. Small differences in thyroid function may be important for body mass index and the occurrence of obesity in the population. J Clin Endocrinol Metab. 2005;90(7):4019-24.
8. Cheng S, Massaro JM, Fox CS, et al. Adiposity, cardiometabolic risk, and Vitamin D Status: The Framingham Heart Study. Diabetes 2010;59:242-248.
9. Grundy SM, Brewer HB Jr, Cleeman JI, et al; American Heart Association; National Heart, Lung, and Blood Institute. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 2004;109:433-8.
10. Geberhiwot T, Haddon A, Labib M. HbA1c predicts the likelihood of having impaired glucose tolerance in high-risk patients with normal fasting plasma glucose. Ann Clin Biochem. 2005;42:193-5.
11. Grant T, Soriano Y, Marantz PR, et al. Community-based screening for cardiovascular disease and diabetes using HbA1c. Am J Prev Med 2004;26:271-5.
12. Jones ME, Schoemaker M, Rae M, et al. Changes in estradiol and testosterone levels in postmenopausal women after changes in body mass index. J. Clin Endocrinol Metab, 2013;98(7):2967-2974.
13. Yassin A, Doros G. Testosterone therapy in hypogonadal men results in sustained and clinically meaningful weight loss. Clin Obesity 2013;3:73-83.
14. Kargi AY, Iacobellis G. Adipose tissue and adrenal glands: novel pathophysiological mechanisms and clinical applications. Int J Endocrinol. 2014;2014:614074